Autores: Avelar SOS, Bretas CG, Carvalho LMA,
Kelles SMB, Mendonça ICA, Talim MCT, Alonso J , Cantanheda CRO, Conte T, Furlan LHP , Oliveira CAC, Pagnoncelli A , Menezes VM , Dr. Alexandre Pagnoncelli, Dr Carlos Augusto Cardim de Oliveira, Dra Claudia Regina de O. Cantanheda, Dra. Izabel Cristina Alves Mendonça, Dr. Jurimar Alonso.
Introdução - A reconstrução do ligamento cruzado anterior, por via artroscópica, é um procedimento ortopédico comum, em que se utiliza enxerto de tendão patelar ou de tendão semitendinoso ou grácil. A fixação destes enxertos é feita com o uso de parafusos de interferência metálicos ou bioabsorvíveis.
Kelles SMB, Mendonça ICA, Talim MCT, Alonso J , Cantanheda CRO, Conte T, Furlan LHP , Oliveira CAC, Pagnoncelli A , Menezes VM , Dr. Alexandre Pagnoncelli, Dr Carlos Augusto Cardim de Oliveira, Dra Claudia Regina de O. Cantanheda, Dra. Izabel Cristina Alves Mendonça, Dr. Jurimar Alonso.
Introdução - A reconstrução do ligamento cruzado anterior, por via artroscópica, é um procedimento ortopédico comum, em que se utiliza enxerto de tendão patelar ou de tendão semitendinoso ou grácil. A fixação destes enxertos é feita com o uso de parafusos de interferência metálicos ou bioabsorvíveis.
Os parafusos de interferência bioabsorvíveis foram introduzidos na década de 1990, tendo como vantagem descrita em relação aos parafusos metálicos, a possibilidade de facilitar uma eventual revisão cirúrgica, já que, uma vez absorvidos, dispensariam a etapa de remoção do parafuso. Seriam mais adequados, também, nos procedimentos de acompanhamento radiológico no pós-operatório, por não provocarem artefatos à ressonância magnética.
Além disto, poderiam representar menores riscos de laceração do enxerto com a mesma capacidade de fixação.
Objetivos – Estabelecer, através de revisão da literatura, se os benefícios esperados se confirmaram ao longo dos anos.
Métodos – Foi realizada busca no Medline, via PubMed, de revisões sistemáticas e ensaios clínicos randomizados publicados nos últimos cinco anos. Buscou-se, também, levantar séries de casos e relatos de casos, com o objetivo de se conhecer possíveis efeitos adversos relacionados a esta técnica.
Resultados – Foram encontrados uma revisão sistemática e cinco ensaios clínicos randomizados publicados nos últimos cinco anos, com amostras pequenas, mas com resultados consistentes. Um ensaio clínico não randomizado mostrou resultados semelhantes aos randomizados. Os relatos de casos servem como alerta para a possibilidade de efeitos adversos, que geralmente não são demonstrados nos ensaios clínicos.
Conclusão – Os estudos não demonstram benefícios clínicos ou funcionais adicionais dos parafusos absorvíveis. Houve ainda maior ocorrência de dor com a utilização destes, e as vantagens em relação à simplificação da técnica em casos de revisão são questionáveis, pelo lento processo de degradação e pelo processo inflamatório causado (cistos, pseudo-abscessos e migração dos parafusos). Não há evidências que justifiquem o uso preferencial
rotineiro dos sistemas de fixação absorvíveis ou que justifiquem seus custos
superiores.
Recomendação – Tendo em vista que os estudos clínicos randomizados comparando as técnicas de fixação de enxerto com parafusos absorvíveis e metálicos, não demonstraram superioridade dos parafusos absorvíveis em relação a desfechos clínicos e que a relação custo-efetividade ainda é desconhecida em nosso meio, a Câmara Técnica Nacional de Medicina Baseada em Evidências NÃO recomenda a incorporação dos sistemas de fixação absorvíveis em pacientes submetidos à reconstrução de ligamento cruzado anterior.
1. Questão Clínica
a) Há benefícios adicionais em termos de segurança e eficácia no uso de Parafusos Bioabsorvíveis para fixação femoral em Reconstrução de LCA com tendão patelar ou tendões flexores comparado ao uso de parafusos não absorvíveis?
b) Há benefícios adicionais em termos de segurança e eficácia no uso de Parafusos Bioabsorvíveis para fixação tibial em Reconstrução de LCA com tendão patelar ou tendões flexores comparado ao uso de parafusos nãoabsorvíveis?
2. Introdução
2.1. Aspectos epidemiológicos
A função do ligamento cruzado anterior (LCA) é a prevenção do deslocamento anterior da tíbia. O LCA costuma ser o ligamento mais comumente lesado e estar associado com o dano ao menisco ou com o ligamento medial colateral.

O sinal clínico característico da ruptura do LCA é o sinal da “gaveta” positivo, quando o joelho é flexionado a 90 graus e tracionado anteriormente, apresentando importante aumento da amplitude de movimento da articulação.

O LCA é o ligamento responsável pela estabilidade rotacional do joelho.
A lesão pode ocorrer após uma entorse do joelho, sendo mais comum durante atividade esportiva. Os sintomas principais da lesão são dor, derrame articular no joelho e impotência funcional. O tratamento na fase aguda consiste de antiinflamatórios, gelo, repouso e fisioterapia. O paciente com o LCA lesado consegue correr em linha reta, andar, nadar, porém ao praticar atividade na qual necessite "girar" sobre o joelho, vai sentir o joelho instável e terá grande chance de vir a ter novos entorses.
O manejo cirúrgico costuma ser indicado para pacientes com instabilidade articular e prejuízo de atividades diárias.
A reconstrução artroscópica do ligamento cruzado anterior (LCA) consiste no procedimento ortopédico cirúrgico mais comum atualmente.
Alguns tipos de enxertos têm sido utilizados na reconstrução do LCA como: o tendão patelar, os tendões flexores do joelho (semitendíneo e grácil) também chamados de isquiotibiais ou semitendinosos (“hamstring technique”), tendão quadriciptal ou tendão de cadáver 1.

As técnicas que utilizam o tendão patelar ou os tendões flexores proporcionam resultados clínicos e funcionais semelhantes, como foi demonstrado em vários ensaios clínicos randomizados. Estes resultados são satisfatórios em 85 a 90% dos pacientes 2,3,4,5,6,7.
Entretanto, no que se refere às técnicas de fixação do enxerto ainda existe alguma discussão.
A técnica mais comum de fixação utiliza parafusos de interferência metálicos, que podem ser usados tanto para fixação de enxertos patelares quanto nos semitendinosos 8.
As vantagens dos parafusos de interferência metálicos incluem fixação efetiva e confiável dos enxertos próximos à linha articular, com redução dos riscos de movimentação do enxerto dentro dos túneis ósseos e do alargamento destes túneis. 9,10
Desvantagens potenciais destes parafusos têm sido descritas como laceração das suturas, do enxerto e perda do plug ósseo durante a inserção. 11, 12, 13 Mas, a principal razão pela qual o uso dos parafusos metálicos nas intervenções de reconstrução do LCA tem sido questionado foi a dificuldade de remoção dos mesmos nos eventos de revisão cirúrgica, e os possíveis artefatos provocados nas imagens de ressonância magnética, quando há necessidade deste tipo de avaliação no pós-operatório. 14
Estes fatores levaram ao interesse crescente pelos parafusos de interferência bioabsorvíveis, teoricamente capazes de superar as dificuldades acima descritas relacionadas aos parafusos metálicos, com a mesma capacidade de fixação do enxerto. Estes parafusos foram introduzidos nos anos 1990 e, segundo os fabricantes, seriam completamente degradados e absorvidos até dois anos após o implante, permitindo a reposição do tecido ósseo nos sítios tibial e femoral de implante dos mesmos.
Entretanto, a velocidade de absorção destes parafusos depende de uma série de fatores, que incluem a composição dos mesmos, massa, quantidade de cristalização, cobertura da superfície e o ambiente em que são inseridos. 15
2.2. Descrição da tecnologia
Os parafusos de interferência bioabsorvíveis são constituídos por polímeros de ácido poliglicólico (PGA) ou de ácido poliláctico (PLA). Alguns representam associação destes dois ácidos, enquanto outros têm um destes ácidos associados a outros polímeros ou a materiais biocerâmicos como a Hidroxiapatita (HA) ou o fosfato tricálcico (TCP). Geralmente, o ácido poliglicólico tem um processo de absorção mais rápido que o ácido polilático. A absorção destes polímeros pelo organismo é feita através de hidrólise lenta, com liberação, ao final, de CO2 e água.
O processo de degradação no organismo de qualquer um destes materiais não é dependente de atividade enzimática 16, mas pode provocar reações inflamatórias inespecíficas com ativação de fibroblastos, macrófagos e leucócitos polimorfonucleares. Este processo pode durar até cinco anos. 16,17
Existem diversos modelos de sistemas de fixação de tendão absorvíveis sendo comercializados em nosso país para fixação tibial e femoral.
TIBIAIS


FEMURAIS

TIBIAIS E FEMURAIS


Como alternativa existem os sistemas de fixação de enxertos nãoabsorvíveis como os parafusos de interferência metálicos. Alguns modelos em titânio vêm sem bordas, o que previne a laceração do enxerto e não interfere com a resolução das imagens radiológicas à ressonância magnética.
Além destes são comercializados também outros sistemas de fixação não-absorvíveis como parafusos com arruelas em titânio ou aço, pinos transversais em titânio, endobottons em titânio, grampos em titânio e parafusos em polietileno.
TIBIAIS



3. Metodologia
3.1. Bases de dados pesquisadas:
Identificação de avaliações da tecnologia já realizadas por Câmaras Técnicas do Sistema Unimed, Medline via Pubmed, Cochrane, Agências de Avaliação de Tecnologia da INAHTA .
3.2. Palavras-chave ou Descritores (DeCS) utilizados: anterior cruciate ligament, bone screws, absorbable implants, intrafix, rigidifix.
3.3. Desenhos dos estudos procurados:
Metanálises e Ensaios Clínicos Randomizados ou não randomizados.
Na ausência destes, buscou-se também, levantar séries de casos e relatos de casos, com o objetivo de se conhecer possíveis efeitos adversos relacionados a esta técnica.
3.4. População envolvida:
Pacientes submetidos à reconstrução de ligamento cruzado anterior (LCA)
3.5. Intervenção:
Fixação dos enxertos com sistemas de fixação absorvíveis.
3.6. Comparação:
Fixação dos enxertos com sistemas de fixação metálicos.
3.7. Desfechos:
Clínicos (funcionalidade, infecção, dor); desfechos substitutos (laceração de suturas e do enxerto, dificuldade de remoção do implante em revisão cirúrgica, artefatos provocados nas imagens de ressonância magnética no pós-operatório, taxas de reintervenção), alargamento de túneis ósseos, tempo de absorção do parafuso.
3.8. Período da pesquisa:
Últimos cinco anos.
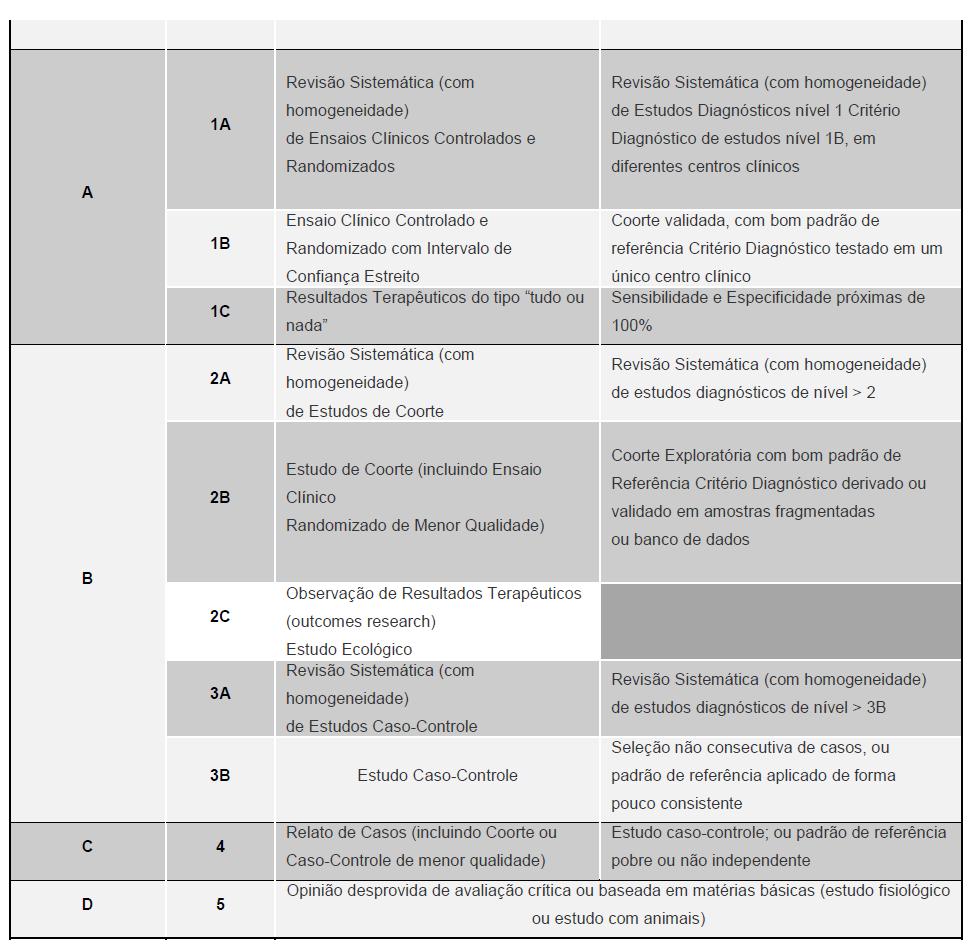
O grau de recomendação tem como objetivos dar transparência às informações, estimular a busca de evidência científica de maior força e auxiliar a avaliação crítica do leitor, o responsável na tomada de decisão junto ao paciente.

4. Resultados
4.1. Comentários
Os resultados, quanto a desfechos clínicos, após a reconstrução cirúrgica do ligamento cruzado anterior são semelhantes, tanto na fixação tibial quanto na femoral, com os dois tipos de fixação utilizados, ou seja, com parafusos de metal ou com parafusos bioabsorvíveis, como já havia sido demonstrado na revisão feita pelos grupos de avaliação de tecnologias do Sistema Unimed 24, 25 em 2005 e 2006 e confirmado pelos ensaios clínicos randomizados mais recentes 20,21,22. Estes ensaios, embora individualmente com amostras pequenas, demonstram resultados bastante semelhantes e, portanto, são consistentes. São ensaios com critérios de exclusão rígidos, incluindo geralmente pacientes com acometimento restrito ao ligamento cruzado anterior, unilateralmente.
As possíveis vantagens do parafuso bioabsorvível quanto à facilitação de revisões cirúrgicas, pela não necessidade de remoção do parafuso são questionáveis, uma vez que a degradação e absorção do parafuso são lentas, durando cerca de quatro anos. Assim, qualquer revisão durante este longo período, necessitará da retirada do parafuso.
Por outro lado, a absorção, mesmo completa do parafuso, não foi acompanhada de reconstituição óssea nos locais onde os mesmos foram colocados 16.
A possibilidade de avaliação através de ressonância magnética no pós-operatório, outro fator apontado como vantagem relacionada ao uso de parafusos de interferência bioabsorvíveis, também pode ser questionada porque resultados semelhantes podem ser obtidos com os parafusos de titânio, que também não prejudicam a avaliação por este método radiológico.
A ressonância magnética, ainda que precisa para verificar o estado do enxerto, pode não ter a mesma precisão em determinar a absorção do parafuso e sua eventual substituição por tecido ósseo, como demonstrado no relato de caso feito por Park e Tibone 17. Estes autores descrevem um caso de nova abordagem cirúrgica motivada por dor e edema sobre a região anterior da tíbia, mais de quatro anos após a reconstrução do LCA. A avaliação através da ressonância no pré-operatório indicava que o parafuso bioabsorvível usado na primeira cirurgia estava intacto. No per operatório constatou-se que não havia resquício do parafuso, sendo curetado material amorfo, compatível com abscesso estéril.
O uso de parafusos biodegradáveis na fixação do enxerto tendíneo seja ele patelar ou semitendinoso, não está isenta de riscos. Como o caso acima mencionado, há descrição de formação de abscessos estéreis pré-tibiais, a partir de cistos, tardiamente após a reconstrução do ligamento cruzado anterior 26. A migração do parafuso, uma complicação inicialmente creditada apenas aos parafusos de interferência metálicos, também foi descrita com parafusos bioabsorvíveis 27,28, sobretudo com aqueles usados para a fixação tibial. A migração do parafuso geralmente é uma intercorrência precoce que ocorre dentro dos primeiros meses após a cirurgia e é causa de dor e de limitação dos movimentos do joelho.
As evidências de que não há benefício clínico ou funcional adicional dos parafusos de interferência bioabsorvíveis em relação aos parafusos metálicos são consistentes e robustas.
As vantagens quanto à simplificação técnica nos casos de revisão cirúrgica são questionáveis diante do curso muito lento do processo de degradação e absorção dos parafusos bioabsorvíveis, implicando que, em muitas revisões cirúrgicas, ocorra a mesma necessidade de remoção destes parafusos que ocorre com os parafusos metálicos. Além disto, o processo lento de absorção implica em reação inflamatória com riscos de formação de cistos, pseudo-abscessos e migração dos parafusos.
Os possíveis benefícios advindos da ausência de artefatos aos exames de ressonância magnética também podem ser usufruídos com o uso de parafusos de titânio.
Não foram encontrados estudos clínicos em humanos comparando o sistema de pinos transversos absorvíveis (Rigidifix ®) ou o sistema de fixação com parafuso e bainha, em polietileno ou absorvível (Intrafix ®) com sistemas de fixação metálicos.
4.2. Avaliação de custos
Os sistemas de fixação ligamentar absorvíveis ou não, apresentam grande variação de preços no mercado.
Relação de Registros na Anvisa e Cotação de Preços

5. Conclusão e recomendações
5.1. Conclusão
Os estudos demonstram os seguintes resultados do emprego de sistemas de fixação absorvíveis para reconstrução de ligamento cruzado anterior em relação ao emprego de sistemas de fixação metálicos:
Não há benefícios clínicos adicionais 18, 20, 21, 29 ;
Não há benefícios funcionais adicionais 18, 19, 22, 23, 29 ;
As evidência são controversas em relação ao retorno à atividade física 19, 20;
Há registros de maior ocorrência de dor com o uso de parafusos absorvíveis 19, 20;
As vantagens em relação à simplificação da técnica em casos de revisão são questionáveis pelo lento processo de degradação e pelo processo inflamatório causado (cistos, pseudo-abscessos e migração dos parafusos) 15, 16, 17, 23;
Não há evidências que justifiquem o uso preferencial rotineiro dos sistemas de fixação absorvíveis ou que justifiquem seus custos superiores;
5.2. Recomendação da Câmara Técnica Nacional de Medicina Baseada em Evidências (CTNMBE):
Tendo em vista que os estudos clínicos randomizados comparando as técnicas de fixação de enxerto com parafusos absorvíveis e metálicos, não demonstraram superioridade dos parafusos absorvíveis em relação a desfechos clínicos e que a relação custo-efetividade ainda é desconhecida em nosso meio, a Câmara Técnica Nacional de Medicina Baseada em Evidências NÃO recomenda a incorporação dos sistemas de fixação absorvíveis em pacientes submetidos à reconstrução de ligamento cruzado anterior.
6. Referências Bibliográficas:
1. Sociedade Brasileira de Cirurgia de Joelho. Enquete. Disponível em
http://www.sbcj.org.br/sbcj.cfm?cmt=1&p1_enq=1461429&categ_id=1208885&env=1 .
Acesso em 06/12/2008.
2. Aglietti P, Giron F, Buzzi R, Biddau F, Sasso F. Anterior cruciate ligament reconstruction: bone-patellar tendon-bone compared with double semitendinosus and gracilis tendon grafts. A prospective, randomized clinical trial. J Bone Joint Surg Am. 2004 Oct;86-A(10):2143-55.
3. Beynnon BD, Johnson RJ, Fleming BC, Kannus P, Kaplan M, Samani J, Renström P.
Anterior cruciate ligament replacement: comparison of bone-patellar tendon-bone grafts with two-strand hamstring grafts. A prospective, randomized study. J Bone Joint Surg Am. 2002 Sep;84-A(9):1503-13.
4. Ejerhed L, Kartus J, Sernert N, Köhler K, Karlsson J. Patellar tendon or semitendinosus tendon autografts for anterior cruciate ligament reconstruction? A prospective randomized study with a two-year follow-up. Am J Sports Med. 2003 Jan-Feb;31(1):19-25.
5. Eriksson K, Anderberg P, Hamberg P, Löfgren AC, Bredenberg M, Westman I, Wredmark T. A comparison of quadruple semitendinosus and patellar tendon grafts in reconstruction of the anterior cruciate ligament. : J Bone Joint Surg Br. 2001 Apr;83(3):348-54.
6. Jansson KA, Linko E, Sandelin J, Harilainen A. A prospective randomized study of patellar versus hamstring tendon autografts for anterior cruciate ligament reconstruction. Am J Sports Med. 2003 Jan-Feb;31(1):12-8.
7. Laxdal G, Kartus J, Hansson L, Heidvall M, Ejerhed L, Karlsson J. : A prospective randomized comparison of bone-patellar tendon-bone and hamstring grafts for anterior cruciate ligament reconstruction. Arthroscopy. 2005 Jan;21(1):34-42.
8. Kurosaka M, Yoshiya S, Andrish JT. A biomechanical comparison of different surgical techniques of graft fixation in anterior cruciate ligament reconstruction. Am J Sports Med. 1987;15:225-229.
9. Paschal SO, Seemann MD, Ashman RB, Allard RN, Montgomery JB. Interference fixation versus postfixation of bone–patellar tendon– bone grafts for anterior cruciate ligament reconstruction: a biomechanical comparative study in porcine knees. Clin Orthop Relat Res. 1994;300:281-287.
10. Clatworthy MG, Annear P, Bulow JU, Bartlett RJ. Tunnel widening in anterior cruciate ligament reconstruction: a prospective evaluation of hamstring and patella tendon grafts. Knee Surg Sports Traumatol Arthrosc. 1999;7:138-145.
11. Bach BB. Potential pitfalls of Kurosaka screw interference fixation for ACL surgery. Am J Knee Surg. 1989;2:76-82.
12. Lemos MJ, Jackson DW, Lee TQ, Simon TM. Assessment of initial fixation of endoscopic interference femoral screws with divergent and parallel placement. Arthroscopy. 1995;11:37-41.
13. Pierz K, Baltz M, Fulkerson J. The effect of Kurosaka screw divergence on the holding strength of bone-tendon-bone grafts. Am J Sports Med. 1995;23:332-335.
14. Shellock FG, Mink JH, Curtin S, Friedman MJ. MR imaging and metallic implants for anterior cruciate ligament reconstruction: assessment of ferromagnetism and artifact. J Magn Reson Imaging. 1992;2:225-228.
15. Radfort MJ, Noakes J, Read J, Wood DG. The natural history of a bioabsorbable interference screw used for anterior cruciate ligament reconstruction with a 4-strand hamstring technique. Arthroscopy 2005;21(6): 707-710.
16. Barber FA, Dockery WD. Long-term absorption of poly-L-lactic Acid interference screws. Arthroscopy 2006;22(8): 820-6.
17. Park MC, Tibone JE. False magnetic resonance imaging persistence of a
biodegradable anterior cruciate ligament interference screw with chronic inflammation
after 4 years in vivo. Arthroscopy 2006;22(8): 911.e1-4.






